In patients with primary angle closure glaucoma and in whom the ciliary body processes were seen on gonioscopy, the axial length, anterior chamber depth, and vitreous length were significantly smaller.
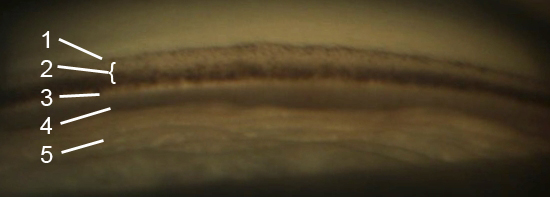
View on gonioscopic examination. The number structures are as follows: 1. Schwalbe’s line, 2. Trabecular meshwork (TM), 3. Scleral spur, 4. Ciliary body, 5. Iris. (Source via CC by 3.0)
Glaucoma is a chronic and common ocular morbidity that is characterized by the progressive loss of retinal ganglion cells. On eye examination, glaucoma is diagnosed by clinical findings of neuroretinal rim thinning and usually increased intraocular pressure (IOP) and by diagnostic tests showing loss of the retinal nerve fiber layer and corresponding visual field defects.
Primary angle closure glaucoma (PACG) is less common than open-angle glaucoma, but the former is more common in the Asian population. Mechanisms of PAC can involve the pupil, ciliary body (CB), lens, or a combination thereof. Predispositions to anterior segment crowding include a shorter axial length (AL), a smaller corneal diameter, increased lens vault and lens thickness, and a lens that is more positioned anteriorly.
Determination of angle closure is usually done clinically via gonioscopy. The ciliary body processes (CBP) is not normally seen on gonioscopy because of total internal reflection, unless there is an existing eye condition (e.g. lens subluxation, aphakia, increased lens thickness). Thus, the visualization of the CBP on gonioscopy is usually indicative of anterior segment crowding.
This prospective clinical study recruited patients with PACG aged 50-80 years, with the objective of studying the difference in ocular biometrics between those with or without visible CBP. Open-angle glaucoma patients served as the control group. Gonioscopy and A-sound biometry were performed on all study patients.
A total of 141 PAC eyes and 32 control eyes were recruited, with the CBP not visualized in all members of the latter. Results showed that there was a significant difference in age between the PAC and control group, likely due to an increased LT and decreased anterior chamber depth (ACD). Females were also more likely to have PAC, which corroborated previous reports that females have a shorter AL and shallower ACD.
Differences in the PACG group were also observed when stratified according to the visualization of the CBP. AL, ACD, and vitreous length (VL) were smaller in patients with PAC and with CBP visualization. However, the relative lens position was not significantly different between the two groups with PACG.
The advantages of this study are the following: (1) all participants were Asian, in which PAC mostly occurs via non-pupillary block mechanisms; (2) none had undergone laser peripheral iridotomy (LPI) to open the angle; and (3) biometric parameters in PAC patients with or without gonioscopic visualization of the CBP were compared.
Supakontanasan, W., Thunwiriya, P., Suwan, Y., Nilphatanakorn, S., Arunmongkol, S., & Teekhasaenee, C. (2019). Effect of Visibility of the Ciliary Body Processes on Ocular Biometric Parameters in Patients with Primary Angle Closure. Japanese Journal of Ophthalmology. doi: 10.1007/s10384-019-00686-3